


Introduction
Healthcare leadership experienced immense and unprecedented strain during the novel coronavirus 19 (COVID-19) pandemic. Surgical specialties, in particular, were faced with the dual strains of shifting clinical priorities and significantly reduced case volumes, with both financial and clinical impacts.1,2 Indeed, one study found a 65% reduction in emergency general surgery operative volume.3 As was the case with physicians of a variety of specialties, surgeons were thrust into a new role during the pandemic, during which crisis leadership took a central role in healthcare organizations.4
Much of the healthcare leadership literature is modeled on the business world, emphasizing the efficacy of various leadership styles in different scenarios. In the academic healthcare setting, leadership often consists of trust building, reflection, planning for the future, and ensuring the trust and well-being of employees.5 However, unlike the business sphere, a healthcare leader is not analogous to a manager.6 On the contrary, healthcare leaders are challenged to have vision, drive, and a focus on a broad view of the organizational goals while maintaining clinical excellence.6
Of the existing literature related to healthcare crisis leadership, focus is largely placed on leadership styles, again adapted from the field of business. Most such papers are qualitative, narrative, or opinion pieces, and high-quality data is lacking in this field. Leadership styles can be broadly defined as autocratic, bureaucratic, charismatic, transformational, laissez-faire, transactional, supportive, and democratic.7
However, compared to standard leadership, crisis leadership requires a disparate skillset, with faster reaction time and impact, significantly more uncertainty and stress, and a strong emphasis on operational changes.6,8 In addition, a growth mindset becomes even more crucial in times of crisis.9 Crisis leadership is characterized by effective and open communication, appropriate resource prioritization, collaboration and trust-building, and functional competency.10,11 Qualities of the effective crisis leader have been described as courage, accountability, determination, and the ability to remain calm yet adaptive and decisive under stress.8,10 Competency is poorly studied in the crisis management literature.12 However, according to Forbes, the most effective crisis leadership style is transformational, with the ability to focus on the “big picture.”13
While surgical leadership has been defined in three domain (feedback, training, and atmosphere), crisis leadership has not been specifically studied in surgeons, and surgeons do not systematically receive formal leadership training.14 In crisis situations, a multitude of individuals are involved at various levels of the hierarchy.11 As with all physicians, the credibility assigned to the individual based solely on their clinical position can result in the perception that these clinicians would be ideal leaders.15 Indeed, choosing leaders based on expertise has been demonstrated to inspire confidence and result in more efficacious leaders.15
Surgeons are well-placed to develop leadership skills given the roles they hold on the surgical team, and, in the cases of healthcare crises such as COVID-19, surgeons must put their leadership skills to the test in order to facilitate safe and effective care for the surgical patient. The American College of Surgeons has noted that the modern surgical leader must engage a team-based approach to success, contrary to the authoritative surgical leadership of the past.16 Literature supports this, with increased confidence in leaders who seek opinions or feedback.17 However, to our knowledge, there are no studies surveying surgeons regarding their opinions of surgical and healthcare leadership during the COVID-19 pandemic. Therefore, the aim of this study was to evaluate surgeon perspectives on leadership strategies during the COVID-19 pandemic.
Methods
Data Collection
A nationwide survey-based assessment of surgeons’ perspectives on leadership was performed. A list of possible survey questions was generated from interviews with 25 surgeons from different specialties and institutions. The survey was then piloted among a different group of 10 surgeons and survey questions were modified based on the collected feedback.
A final questionnaire consisting of 30 questions [25 multiple-choice, 3 open-ended, 2 Likert-scale (1-5, 1 = strongly disagree, 5 = strongly agree)] (Supplement 1), was distributed nationwide from November 1, 2022 - January 31, 2023, to publicly available, institutional email addresses of surgeons who were members of the American College of Surgeons.
The survey response tool was set up such that each participant was able to respond only once to the survey. Participation in the survey was voluntary, and no compensation was provided. Anonymity was ensured by not collecting any personal identifiers. Researchers were blinded to the respondent’s institution. Completing the survey served as a consent to participate in the study. This study was considered exempt from our Institutional Review Board.
Data Analysis
Only surveys with >80% of items completed were included in the analysis. Data was described with counts and percentages, mean and standard deviation (SD) and median and interquartile range (IQR), as appropriate. For Likert scale data, responses of “Agree” or “Strongly Agree” were considered as affirmative, while “Disagree” or “Strongly Disagree” were considered negative. Free-text responses from open-ended questions were independently coded and the resulting nominal data presented as percentage of responses per category. The Pearson Chi-square test was used to determine the relationship between nominal scale variables. The Mann-Whitney rank sum test was used to compare ordinal scale variables. Statistical significance was accepted at α = 0.05 and all tests were two-sided. Data was analyzed using SAS software, version 9.4 (SAS Institute®, Cary, NC, USA).
Results
Sample Characteristics
Over the three-month data collection period, 671 of 2360 surveys were completed (28.4% response rate).
The largest proportion of respondents were between the ages of 40-49 (280, 41.7%) and identified as white (419, 62.4%), which is reflective of the overall cohort of surgeons in the United States.18 Compared to the overall population of surgeons, females were slightly overrepresented in our cohort (259, 38.6%).18 Most respondents reported practicing in the Northeast (264, 39.93%) or Midwest (141, 21.0%), in an academic practice (490, 73.0%). A wide range of surgical specialties were represented, with the most being trauma/acute care (168, 25.0%) and general surgery (151, 22.5%). Complete respondent demographic and practice information is noted in Table 1.
Inclusion in Crisis Response
Most respondents (569/671, 84.8%) were not offered formal training or education in crisis management during the COVID-19 pandemic. When queried, only 51.4% (345/671) of participants were asked to provide any input to their institution regarding clinical protocols during the COVID-19 pandemic, and only 36.8% (247/671) were asked to give any feedback on the practice changes that were implemented. Additionally, only 37.1% (249/671) reported that their practice completed a review of the institutional response to the pandemic. The majority of participants (486/671, 72.5%) reported a perceived lack of the opportunity to provide periodic, structured, and anonymous assessments of their leader’s performance during the pandemic.
Crisis Leadership
Our respondents reported that the most common leadership styles embraced by their institutions during the COVID-19 pandemic were bureaucratic (205/671, 30.7%), followed by autocratic (184/671, 27.5%), and supportive (157/671, 23.4%). Other less embraced styles were laissez-faire, transformational, charismatic, transactional, and democratic (Figure 1). On Chi-square testing, there were no differences in responses between practice settings or geographic area.

Contrary to these results, respondents indicated that their optimal perceived leadership style in crisis situations is supportive (231/663, 34.8%), followed by transformational (173/663, 26.1%), and charismatic (80/663, 12.1%) (Figure 2). There were no differences in response by sex, race, or age.

The majority of surgeons (452/671, 67.4%) reported that their surgical leaders did not change their leadership style during the COVID-19 pandemic. Of those that did report a change in leadership style (204/671, 30.4%), all reported adoption of a supportive leadership style, most commonly from the bureaucratic style (122/205, 59.5%).
Leadership Traits
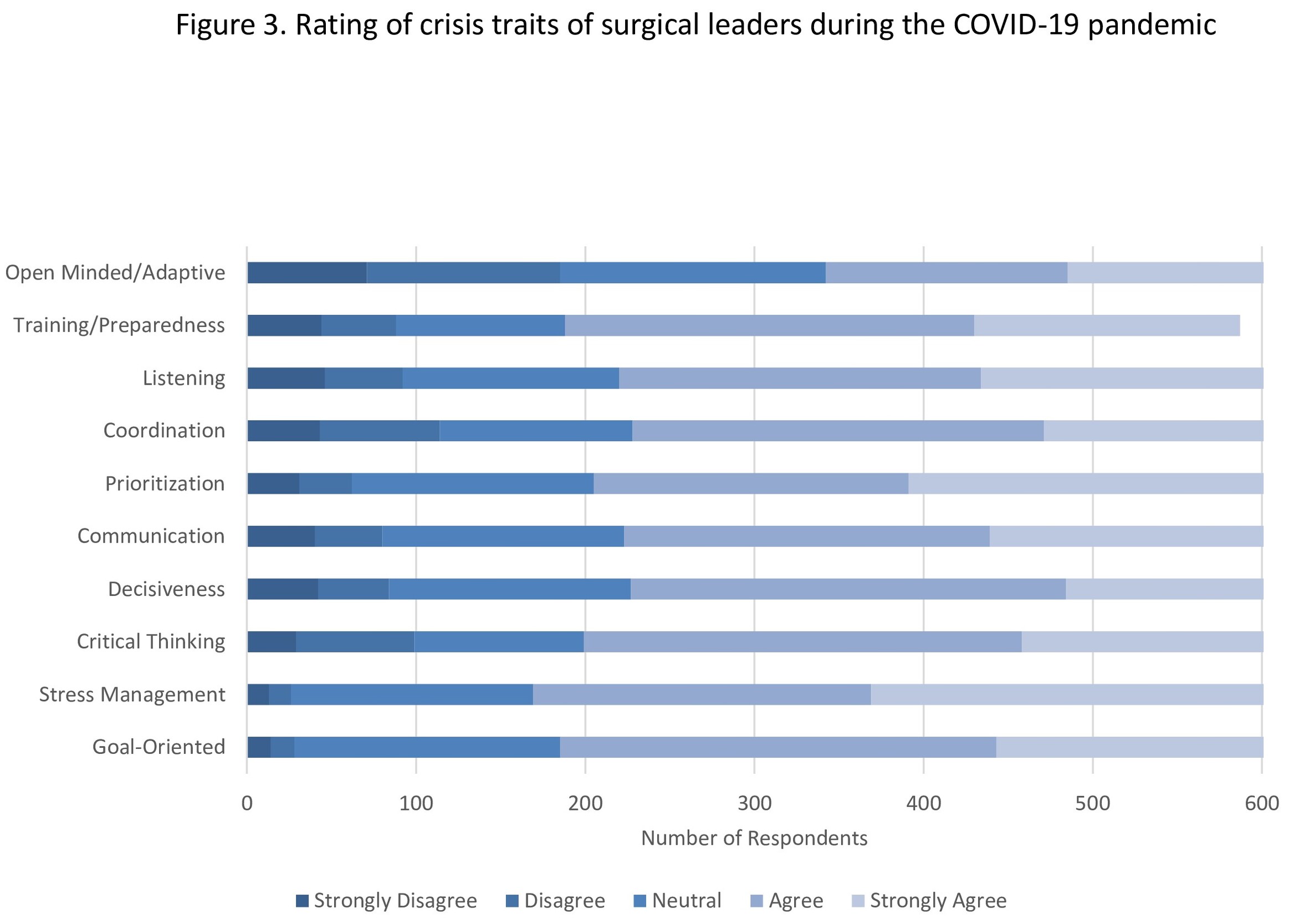
When asked to rate the utility of crisis leadership traits demonstrated by their surgical leader during the COVID-19 pandemic, participants most commonly reported goal-oriented leadership (4.0/5 on a Likert scale) and stress management (4.0/5), followed by critical thinking (3.8/5), decisiveness (3.8/5), communication skills (3.8/5), and prioritization (3.8/5) (Figure 3). The least commonly reported traits were open mindedness and adaptability (3.4/5), training and preparation (3.5/5), and ability to listen (3.6/5). Results did not differ significantly between different demographic groups, geographic area, practice setting, or specialty.

Preparedness for Future Crises
Approximately half of participants (343/671, 51.1%) feel that their practice’s overall preparedness for future major crises has improved because of the COVID-19 pandemic experience. Sixty-two participants (9.2%) shared the advice they would provide to their current leader to improve organizational leadership, in the form of free response questions. These results were analyzed using thematic analysis as described above. The most common theme was listening to feedback from organization members (49/62, 79%), followed by compassion (18/62, 29.1%), and flexibility (13/62, 21%) (Figure 4).

At an institutional level, the most recommended approach by respondents for leadership during future crises of a magnitude comparable to the COVID-19 pandemic was creation of a crisis leadership council (4.7/5 on a Likert scale), creation of a network of teams operating outside of the existing hierarchy and bureaucratic structures (4.4/5), creation of a military-style command structure (4.2/5) and instituting meta-leadership framework (4.0/5) (Table 2).
Discussion
In this survey-based study of United States surgeons, most were not solicited for involvement in, or feedback on, COVID-19 related institutional protocols, and the vast majority (84.8%) were not provided with any crisis leadership training. When polled, most surgeons reported that their surgical leaders used bureaucratic or autocratic leadership methods, however, most respondents felt that the ideal healthcare leadership styles in times of healthcare crisis were supportive and transformational. This is congruent with current literature on crisis leadership, in which the transformational leadership style has been deemed most effective, due to the ability to focus on overarching goals.13 However, there are proponents of more rigid leadership styles in times of crisis, specifically the military leadership model, which falls largely into the autocratic and bureaucratic methods most displayed by surgical leaders in this study.19 The military leadership model involves an operationalized model of task-specific teams integrated into the existing hierarchy, while maintaining a central decision maker.19,20
Our results suggest that most surgical leaders embraced a bureaucratic style during the COVID-19 crisis, while most surgeons preferred their leaders to be supportive during crisis situations. This discrepancy between reported and preferred crisis leadership styles points to a need for targeted leadership training for healthcare leaders.
Similar to the current crisis leadership literature, participants reported goal-directed practice, stress management, critical thinking, decisiveness, communication skills, and appropriate prioritization as the most common crisis leadership traits.8,13 Contrary to previously published studies, trust and transparency were not specifically identified as themes.8,13 In conditions such as that created by COVID-19, these crisis management skills become even more critical, requiring flexibility in the face of rapidly changing information, evidence, and recommendations.12
Effective response in times of crisis requires preparation, rather than waiting for a crisis to strike.9 Additionally, effective institutional crisis leadership increases employee buy-in and willingness to provide care in these difficult situations.10 Therefore, crisis leadership framework should include continual evolvement to prepare for future emergencies.21,22 We suggest that our results should be utilized in the healthcare context to prepare and train the next iteration of surgical leaders.
Our study demonstrates that most surgeons were not provided with specific leadership training related to the COVID-19 pandemic. The current paradigm of healthcare training does not prepare healthcare workers to be leaders, and, importantly, leadership competencies are very different than clinical competencies.23 Additionally, leadership requires team-based performance, while typical healthcare practitioner training aims to maximize individual performance.23 While leadership skills can be taught, developed, and improved to the point of competence, times of crisis do not represent the ideal environment for this sort of learning.17
While the current generation of surgical leaders did not have the benefit of formalized leadership training during their surgical education, it would be prudent to consider incorporation of such training into surgical residency, which does not currently require any leadership training.24 Optimal leadership development has been shown to occur with frequent, early career opportunities to develop leadership skills, and surgical residency provides an ideal environment for this type of supervised leadership practice.14,17 Specific leadership skills that are lacking in current surgical education paradigms include networking and negotiation.17 Notably, communication and prioritization were identified by our study respondents as frequently demonstrated leadership traits in their institutional surgical crisis leadership, supporting their incorporation into surgical leadership training.
During times of crisis, real-time evaluation and feedback can improve the leadership efficacy and provider trust in the leadership structure.14 Specifically in the field of surgery, leadership skills improve with frequent, real-time feedback, classically used to improve proficiency in the operating room, and this paradigm can also be translated to developing as a healthcare leader.14 The use of such a paradigm not only improves leadership efficacy but also providers’ faith in the leadership structure.14 Despite this, our results demonstrate that feedback is not formalized into the system, which fosters a bureaucratic or autocratic leadership method, in which the opinions of the team members are not considered or considered secondary to the leaders’ determinations. Our results suggest that formalized feedback processes should be introduced into the healthcare leadership structure.
This study has several limitations. First, as a survey-based study, response bias is possible, though our demographic breakdown was overall consistent with the population of surgeons in the United States. Second, there are no validated surveys evaluating leadership styles, particularly crisis leadership, therefore, our survey was developed based on institutional provider input and expert consensus. Third, we did not distribute the survey to the surgical leaders themselves because it would have required a significant number of different questions. However, determining their perspective on leadership during COVID-19 pandemic is very important, and we are planning investigate it in a separate, future study. Finally, our results queried a variety of surgical specialties and may not be generalizable to all healthcare workers or surgeons. These limitations notwithstanding, we believe our findings provide meaningful insights into the surgeons’ perspectives on leadership during the COVID-19 pandemic.
Conclusions
Despite the practice of healthcare workers taking on leadership roles during times of crisis, surgeons do not receive specific training in this realm, and are not provided with sufficient opportunity to participate or provide feedback for the healthcare crisis leadership system. Surgical training paradigms should consider the addition of formalized leadership training, and surgical leaders should consider adoption of a supportive or transformational leadership styles during times of crisis, particularly focusing on obtaining input and feedback, and thus building trust and connections with the surgical team.
Disclosure
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.