

INTRODUCTION
The costs of attending medical school in the United States are very high and continue to rise. According to data from the Association of American Medical Colleges (AAMC),1 the median four-year cost of attendance ranges from $286,454 to $390,848 for the Class of 2025, representing a 4% increase over the previous year. These high costs are associated with increased medical school debt, with 71% of students graduating with $210,000 or more in debt.1
Medical costs aside, medical school admissions in the United States remain very competitive, with roughly 40% of applicants being accepted nationally every year and acceptance rates for individual medical schools being around 5%, forcing many applicants to spend additional years improving their credentials to reapply. Thus, according to AAMC 2024 Matriculating Student Questionnaire,2 which was distributed to U.S. medical students who began their training during the 2024-25 academic year, 74.3% of respondents took at least one gap year, a marked increase from the 57.9% of respondents who reported the same a decade ago. Due to this shift, the average age of first-year medical matriculant increased from 22 in the mid-1990s to 24 in 2024. AAMC data also show that about 25% of applicants every year are reapplicants.
Given this high cost and competitive process, many aspiring medical students in the US continue to explore alternative pathways to earn their degrees, including pursuing a medical education abroad. While there are increasing numbers of US students studying medicine abroad, exact information about how many US students go abroad for medical school is not available currently. According to data from the Institute of International Education’s Open Doors Report,3 the overall number of US students studying abroad in any field has increased by 49% in the 2022-23 academic year to 280,716 students, with 6.1% of them studying health professions. The majority (64%) of US students choose Europe for their studies abroad studies, with 50% percent of them studying in just five countries: United Kingdom, Ireland, France, Spain, and Italy.3
Likewise, studying medicine in Europe has become increasingly popular for US students, especially when it comes to English-taught programs.4
In this review we will explore the benefits of studying medicine in Europe for US students, the impact of such a choice on their careers, and the potential challenges associated with studying medicine abroad.
METHODS
We conducted a comprehensive review focused on European medical school education for international students. Our review included peer and non-peer reviewed literature published between 1980 and 2025, online media articles, online content published by consulting companies, online discussion forums (Quora, Reddit, Student Doctor Network), online blogs, and YouTube videos.
The entire team of authors identified the key literature findings that are summarized in this article. According to VA Boston Healthcare System policy, our literature review study does not require an Institutional Board Review.
RESULTS
European countries are the most common destination for US students given their high-quality education and established healthcare systems.
In Europe there are two medical school pathways:
- Standard 6-year medical school for high school graduates.
These programs are the most chosen and are taught in the national languages of each country, although there are some individual classes that are offered in English.
In recent years, the number of non-UK, European medical schools offering their curriculum entirely in English has increased to 107 schools.5
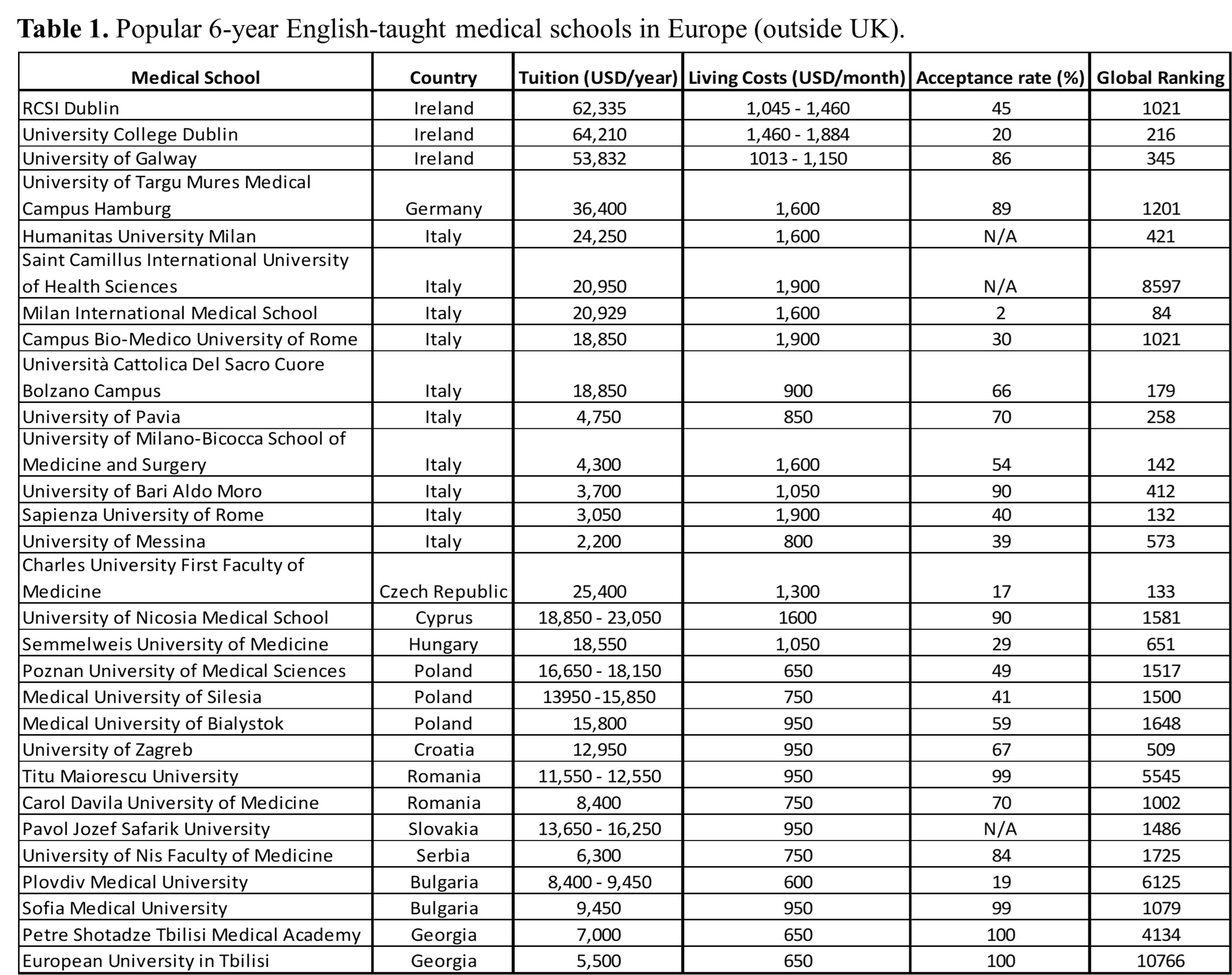
A selection of popular English-taught medical schools for international students, their current ranking, admission rates, tuition, and associated cost of living are presented in Table 1.
- Graduate Entry Programs, which are 4-year programs for students who have already finished their undergraduate studies.
All schools offering these English-taught programs are presented in Table 2.

The benefits and challenges of studying medicine in Europe continue to be debated4–7 and are summarized in Table 3.
Benefits of studying medicine in Europe
- Lower tuition fees and cost of living.
While compared to the US, overall cost associated with medical education is less in European countries (except UK and Ireland), with notable differences between Western and Eastern Europe. Except for Ireland and the United Kingdom, the countries of Western Europe subsidize tuition for their public medical schools, minimizing costs to a few thousand dollars a year. Most public medical schools in Germany and Norway are tuition-free for all students, including those from the United States. However, to take advantage of low and free tuition, US students must prove proficiency in the local language, as medical studies in public universities are taught in the national languages. In comparison, tuition costs in public medical schools are higher in Eastern Europe, ranging from 4 to 18 thousand dollars a year; however, the costs of living are significantly lower than in Western Europe.5
- Higher acceptance rates.
Not only does Europe overall have more and larger medical schools than the United States, but many European medical schools have a dedicated number of spots for international students, thus avoiding competition with local students. Furthermore, the 104 European medical schools that offer an English-taught curriculum (except UK and Ireland)5 are specifically founded for teaching international students. These factors lead to less competition and higher admission rates for US students.
- Flexible admission requirements.
While there are schools with very stringent admission criteria, most medical schools in Europe have more flexible requirements than US medical schools. These can include a lower overall GPA or MCAT scores, optional MCAT requirement, and more intake periods throughout the year. Some schools may require an entrance exam in Chemistry, Biology, Physics, while others do not. Overall, medical schools in Eastern Europe have more flexible admission requirements than those in Western Europe.
- Shorter duration of medical studies.
US students can enroll in a traditional 6-year medical school program in Europe directly after high school, as compared to the United States where students will spend 8-10 years (4 years of undergraduate studies + likely 1 or 2 gap years + 4 years of medical school).
US students with an undergraduate degree can enroll in a 4-year Graduate Entry Program in Europe, without the need for spending one or more gap years waiting for admission to a 4-year US medical school.
Spending fewer years to achieve a medical degree can enable US students to enter the workforce sooner as well as help keep down the overall medical education costs to reduce the debt burden for US students.
- High-quality and globally recognized education.
European universities are renowned for their excellence in medical education. Many medical schools offer rigorous academic programs, modern facilities, cutting-edge technology, research opportunities, and experienced faculty members. Indeed, many European medical schools are highly ranked globally, reflecting a high standard of medical education. This global recognition of European medical qualifications enhances career opportunities for its graduates.
- Multicultural learning experience.
Studying medicine in Europe exposes students to diverse cultures. Interacting with students from various backgrounds enhances the learning experience, fosters cultural competency, improves communications skills, and gives students a global perspective on healthcare. Furthermore, life and experiences outside the classroom, provide students with opportunities to be immersed in the unique culture of their environment.
- Global health exposure.
Attending a medical school in Europe provides students with an opportunity to learn about healthcare systems in different countries and gain clinical experience in diverse settings.
- Clinical experience diversity.
US students studying medicine in Europe will be exposed to different disease patterns, genetic disorders, and environmental and socio-economic determinants of health. This exposure not only will broaden their medical knowledge but will also help them in the future to better understand and treat diverse patient populations.
- Learning a new language.
Regardless of the pathway chosen to study medicine in Europe, living in a new country represents an opportunity to learn and/or improve on a foreign language.
US students who enroll in European public medical schools taught in the local language are required to become proficient in that language prior to starting their medical studies, with many schools offering a preparatory year to learn the local language (source).
Even US students who choose an English-taught medical school in Europe will have the opportunity to learn and practice the local language by interacting with patients, hospital staff, as well as the local population outside the classroom.
- Personal growth and resiliency.
By being away from home and living in a new country, US students inherently step out of their comfort zone and learn to adapt to new environments, manage their own finances, meet new people, and develop different interests and hobbies. These can make students more resilient and contribute to their independence and personal growth.
Challenges of studying medicine in Europe
- The language barrier.
Learning the local language is mandatory for US students who enroll in European public medical schools taught in the local language. While many schools offer a preparatory year to learn the local language, it takes more time and continued efforts to improve the foreign language proficiency. For students enrolled in English-taught programs the language barrier becomes a significant issue when they interact directly with patients and healthcare workers in their local languages. Some schools offer translation services available for patient-learner communication.
- Cultural adjustment.
Adjusting to a new culture, lifestyle, and environment in a different European country and continent can be challenging for US students, potentially affecting their social life, mental health, and academic performance.
- Lack of a support system.
Living and studying in a foreign country away from family and friends can be a challenging experience for many students especially for those who have not travelled to another country alone before. Furthermore, they may not have access to the resources that are accustomed back home. While European schools provide adequate assistance, students may still experience homesickness, loneliness, and cultural shock.
Additionally, making new friends and connections while studying abroad can be a challenge at first and make take some time.
- Complex bureaucracy.
Although the admission requirements for entry into European medical schools are less stringent, the administrative onboarding process and obtaining the necessary visas and residence permits can be complex and time-consuming. This can feel overwhelming to US students unfamiliar with the system.
- Competitive admissions.
While overall medical school admission rates are much higher in Europe than in the US, entering prestigious medical schools in Europe remains highly competitive.
- Cost of living.
The housing costs and other living expenses vary significantly across different European countries. While the overall cost of living is relatively low in Eastern European countries, it can be very high in Western Europe.
- Varying quality of education.
Another disadvantage of European medical schools is the varying quality standards across different countries. While there are exceptional medical schools in Europe, the overall quality of education can vary significantly across different countries and from one school to another, as reflected in school ranking scores shown in Table 1 and Table 2.
- Fewer research opportunities.
While some of the top medical schools offer research opportunities for their students, European medical schools generally place less emphasis on research compared to the US medical schools.
- Varying eligibility for US federal student loans.
According to data from the U.S. Department of Education, there are many European medical schools classified as “eligible” for disbursing federal student loans to US citizens.8 In Europe, almost all the eligible medical schools are in the United Kingdom.
Many other European medical schools are classified as “deferment only” meaning that students cannot use federal loans for their medical school, but any previous student loan can be put into deferred status while attending that medical school.8
- US Licensing requirements.
US students graduating from any foreign medical school must be certified by the Educational Commission for Foreign Medical Graduates (ECFMG) prior to being eligible to apply for residency training and practice in the United States. To become certified by ECFMG, they must pass the United States Medical Licensing Exam® (USMLE) Step 1, Step 2 Clinical Knowledge (CK), and Step 2 Clinical Skills (CS) exams.9
The impact of studying medicine in Europe on US students’ careers
After completing their medical education in Europe, US students embark on taking the USMLE exams that would enable them to obtain the ECFMG certificate and participate in the US residency match. Below we are reviewing how these post-graduation steps are influenced by graduating from a foreign medical school.
Performance on the USMLE exams for ECFMG certification
Every year the USMLE website10 provides data on performance in each of the USMLE exams. The percentage of candidates from US/Canadian and non-US/Canadian medical school that passed Step 1, Step 2 CK, and Step CS of the USMLE between 2012 to 2023 are shown in Table 4.
This data shows that regardless of their country of citizenship, graduates of medical schools outside of the US and Canada have lower pass scores than international medical graduates in all three USMLE exams required for ECFMG certification.
Studies comparing USMLE performance of US citizens graduating from international medical schools (USIMGs) with non-US citizens (non-USIMGs) show that non-USIMGs performed better than USIMGs on the Step 1 and Step 2 CK exams but were outperformed by the USIMGs in the Step2 CS exam.11 Overall, IMGs have also a higher number of USMLE retaking attempts than the US graduates, with US-IMGs having a higher retake number than non-US IMGs.11
Some of the factors contributing to lower scores include differences in the medical school curriculum between the US and foreign schools, variability in student selection criteria, unfamiliarity with the USMLE exam format, and less exposure to US clinical rotations. The language barrier is also considered a contributing factor for non-USIMGs, supported by the fact that non-USIMGs from English-speaking countries perform better than those from non-English speaking countries.11
Despite these differences in USMLE scores, overall USIMGs are significantly more likely than non-USIMGs to eventually achieve ECFMG certification.
Individual performance data are confidential and are provided to each medical school electronically by the ECFMG. Although there is no data in the literature on USMLE performance of individual European medical schools, studies have shown that students who attended medical schools accredited by an agency recognized by the World Federation for Medical Education (WFME) had higher pass rates on the USMLE exams than graduates of medical schools not accredited by a WFME-recognized accrediting body.12
Residency match process
To find a residency training position after obtaining the ECFMG certificate, USIMGs and non-USIMGs must participate, along with graduates of US medical schools, in the yearly residency matching process that is managed by the National Resident Matching Program (NRMP).
Historically, IMGs have faced lower matching rates compared to US graduates and this trend persists according to recent data from NRMP13 as shown in Table 5.
As in previous years, in 2024 the specialties with the highest IMG matching rates were Internal Medicine at 42.5% (31.4% non-USMIG / 11.1% USIMG), Pathology at 37.3% (27.5% non-USMIG / 9.8% USIMG), Family Medicine at 31.7% (15.4% non-USMIG / 16.3% USIMG), Neurology at 29.6% (23.3% non-USMIG / 6.3% USIMG), and Pediatrics at 25.8% (17.7% non-USMIG / 8.1% USIMG).13
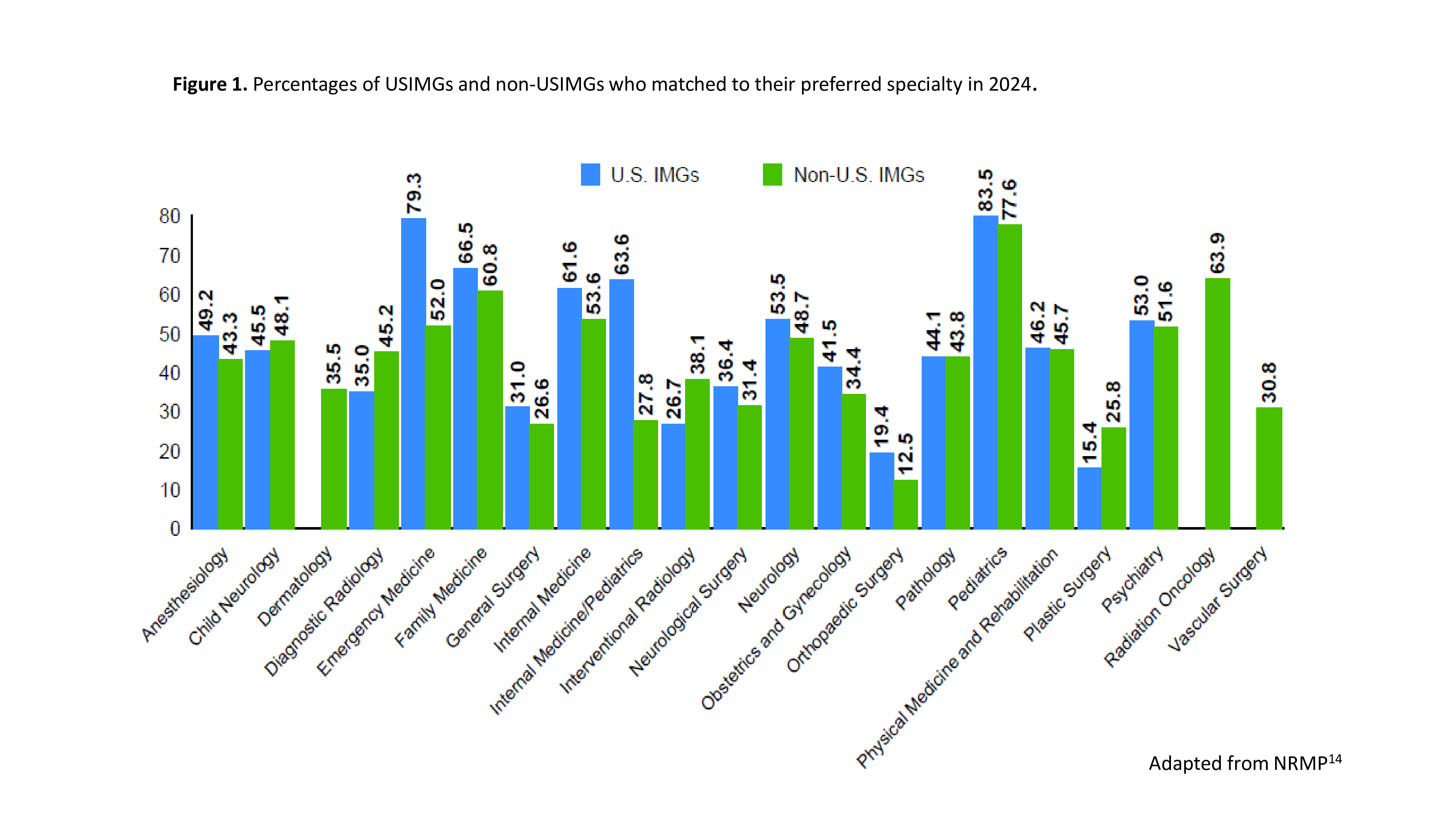
IMGs also have lower probabilities of matching into their preferred specialties than US graduates. Overall, 59.9% of USIMGs and 52.8% of non-USIMGs matched to their preferred specialty in 2024, compared to 89.8% of US graduates.14 The percentages of USIMGs and non-USIMGs who matched to their preferred specialty are shown in Figure 1.

Their 2024 matching rates for general surgery and surgical subspecialties were low, with only 10.3% (5.6% non-USMIG / 4.7 USIMG) matching into a categorical general surgery position.13 However, 46.4% of them matched into non-designated preliminary surgery (NDPS) positions,13 which are one-year positions without the guarantee of a subsequent categorical position. Importantly, studies show that after completing their NPDS year, 37.1% of residents obtain a categorical general surgery position that allows them to complete their surgical training.15 Dedicated and resilient USIMGs and non-USIMGs are eventually able to complete surgical residency training in the US, although it might require more time and research work than the US graduates.16
Although there is no available data on residency matching rates for graduates of individual European medical schools, some schools choose to post this information on their websites. For example, the RSCI medical school in Ireland self-reported a US first round residency match rate of 92% for their class of 2020.17 Participants in online forum discussions perceive that medical schools from United Kingdom, Ireland, and Western Europe are associated with better US residency matching prospects than schools from Eastern Europe, presumably from a greater emphasis on clinical practice and patient interaction as well as higher prestige and recognition in the US.18–20
Some of the reasons for the lower residency match rates for USIMGs include lower scores and multiple attempts on the USMLE exams, unfamiliarity with the electronic residency application system, inadequate understanding of the ranking system, less US clinical experience, and fewer opportunities to obtain letter of recommendations from US clinicians. An additional factor for non-USIMGs is the language barriers that can affect their communication during their interviews.
Another important barrier to securing a residency training position is stigma against those who have studied medicine abroad. Although there is abundant evidence on stigma against non-USIMGs, US students who attend medical school abroad are also stigmatized as being not competitive enough to get into an American medical school.6 However, contrary to the unfounded belief that most US citizens who attend foreign medical schools do so only after several unsuccessful attempts to gain admission to a US school, studies have shown that the majority of USIMGs did not apply to a US medical school prior to studying medicine abroad.21
Despite these challenges, USIMGs and non-USIMGs go on to have fulfilling careers in the US. They contribute significantly to the US healthcare system by comprising 25% of the US physician workforce.22 Compared to US medical graduates, IMGs disproportionally provide care in underserved areas and communities.22–24 However, they also make important contributions to clinical practice, research, innovation, education, and leadership.24,25
CONCLUSIONS
In an era of increasing costs and competition for obtaining a medical degree, studying medicine in Europe can be a valuable opportunity for many US students, offering lower-cost and high-quality education, global recognition, and an enriching cultural experience. However, pursuing a medical degree in Europe has advantages, challenges, and career implications that should be carefully considered for a well-informed decision. Furthermore, Europe is a very diverse continent with many countries, each with their own medical education system, economic environment, geography, language, and culture. As such, thorough research and careful planning are crucial for a successful medical education in Europe.
ACKNOWLEDGMENT
We thank Eliora M. Kristo for assisting with the literature review and her technical assistance with the tables and figures.