Introduction
The coronavirus disease 2019 (COVID-19) pandemic has deeply impacted our society and caused unprecedented disruptions to the personal life and the educational experience and of the general surgery residents. From concerns about personal and familial risk of coronavirus infection, heavy workload, post-traumatic stress, burnout, and COVID-19-related stigma, to reduced operative experience, transition to online platforms for didactic teachings, and decreased preparedness for going into practice, the general surgery residents have been facing significant challenges during the COVID-19 pandemic.1–6
As a result of these significant disruptions, general surgery residents have developed post-traumatic growth and new perspectives following a major crisis such as the COVID-19 pandemic.6 Changes in careers plans because of the pandemic are possible, and have been reported in nurses, medical students, nurses, and medical trainees.7–10 It remains undetermined whether, as part of their new perspectives as a result of the COVID-19, general surgery residents are planning any career changes.
The COVID-19 pandemic has also significantly impacted the financial situation of patients, their families, and our healthcare systems.11 There is little known however, how the pandemic has financially affected the general surgery residents.
The objective of this study is to evaluate the perspectives of general surgery residents on the impact of the COVID-19 pandemic on their financial wellness and career plans.
Methods
A nationwide survey-based assessment of the financial support and salary expectations of general residents was performed. A list of possible survey questions was generated from interviews with 20 general surgery residents from different institutions. Survey validity was assessed by 30 minutes focus group session with 10 general surgery residents. The survey was piloted among a different group of 10 general surgery residents and survey questions were modified based on the collected feedback. After the survey was approved by the Research Committee of the Association of Program Directors in Surgery (APDS), a final questionnaire consisting of 30 questions (19 multiple-choice; 8 yes/no; 3 open-ended) (Supplement), was electronically distributed by the APDS to their membership in May 2020. Program directors willing to have their trainees participate in the survey would then distribute it to their residents. With the APDS approval, we emailed a reminder to the individual general surgery residency program directors in September 2020.
All data was collected in accordance with the requirements of our Institutional Review Board.
Participation in the survey was voluntary, and no compensation was provided. Anonymity was ensured by not requiring any personal identifiers. Participants were informed in writing that by answering the questions and returning the survey, they were providing and documenting their willingness to participate.
Only surveys with >80% of items completed were included in the analysis. Results were calculated based on the number of responses received to each individual question. Free-text responses from open-ended questions were independently coded and the resulting nominal data are presented as percentage of responses per category.
Statistical data was analyzed using SAS data analysis software, version 9.4 (SAS Institute®). The Chi-square test was used to measure the relationship between nominal scale variables. The Mann-Whitney rank sum test was used to compare ordinal scale variables. Statistical significance was accepted at p ≤ 0.05 and all tests were two-sided.
Results
A total of 419 general surgery residents completed the survey. The response rate could not be calculated because the method of distribution of our survey did not allow us to know how many general surgery residency program directors decided to distribute the survey to their residents.
Survey respondent demographics are described in Table 1. Respondents were mostly age 30-39 (55.1%), male (53.6%), single (53.9%), and white (63.1%). The majority of respondents trained in the Northeast (46.5%) and Midwest (29.3%), with a minority from the Southeast (12.2%), Southwest (6.7%) and West (5.3%). Respondents were distributed among PGY-levels (12.7-23.8%).
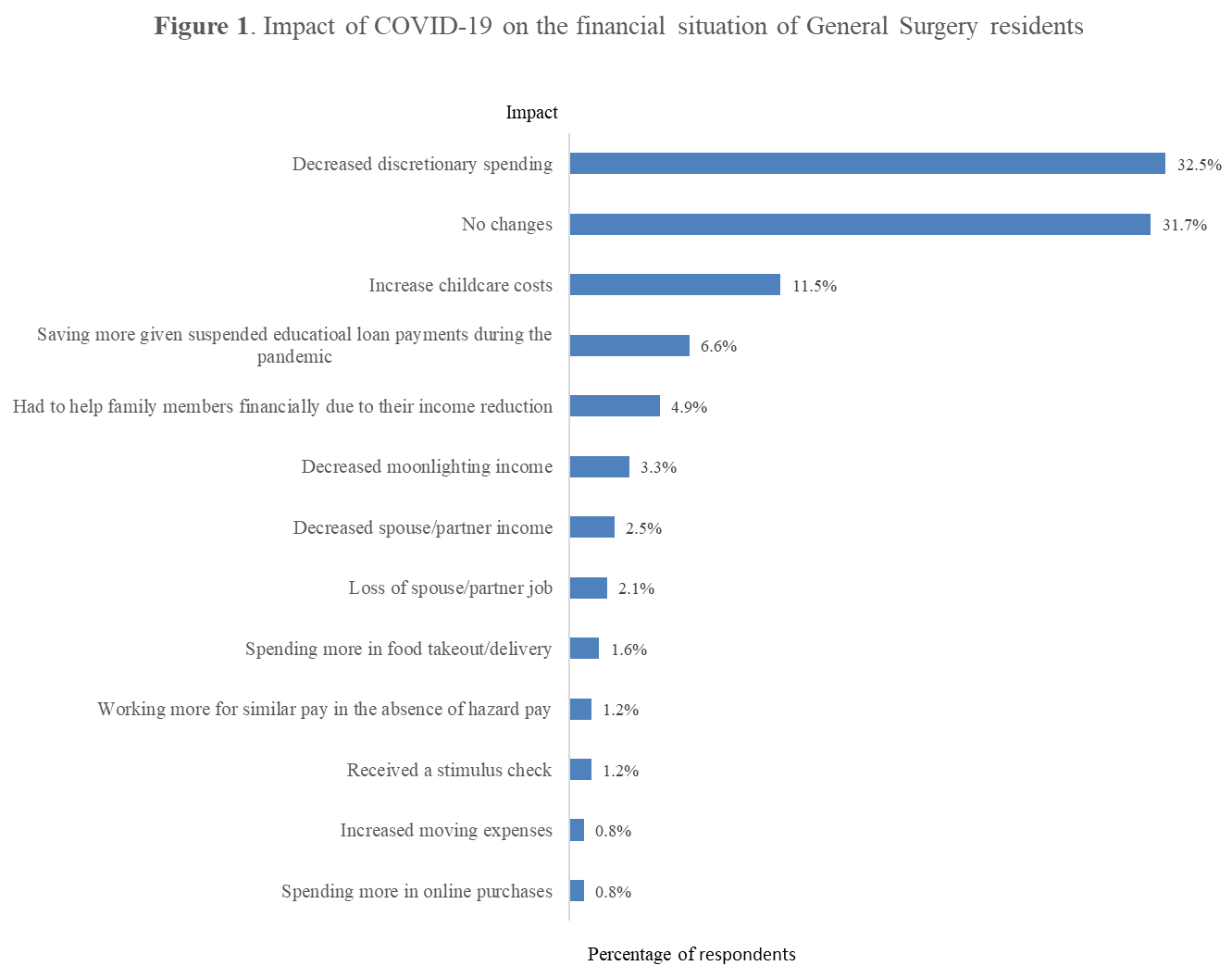
Nearly one third of respondents (32%, n=79) reported that the COVID-19 pandemic decreased discretionary spending, with 32% (n=77) reporting no change in financial situation (Figure 1).

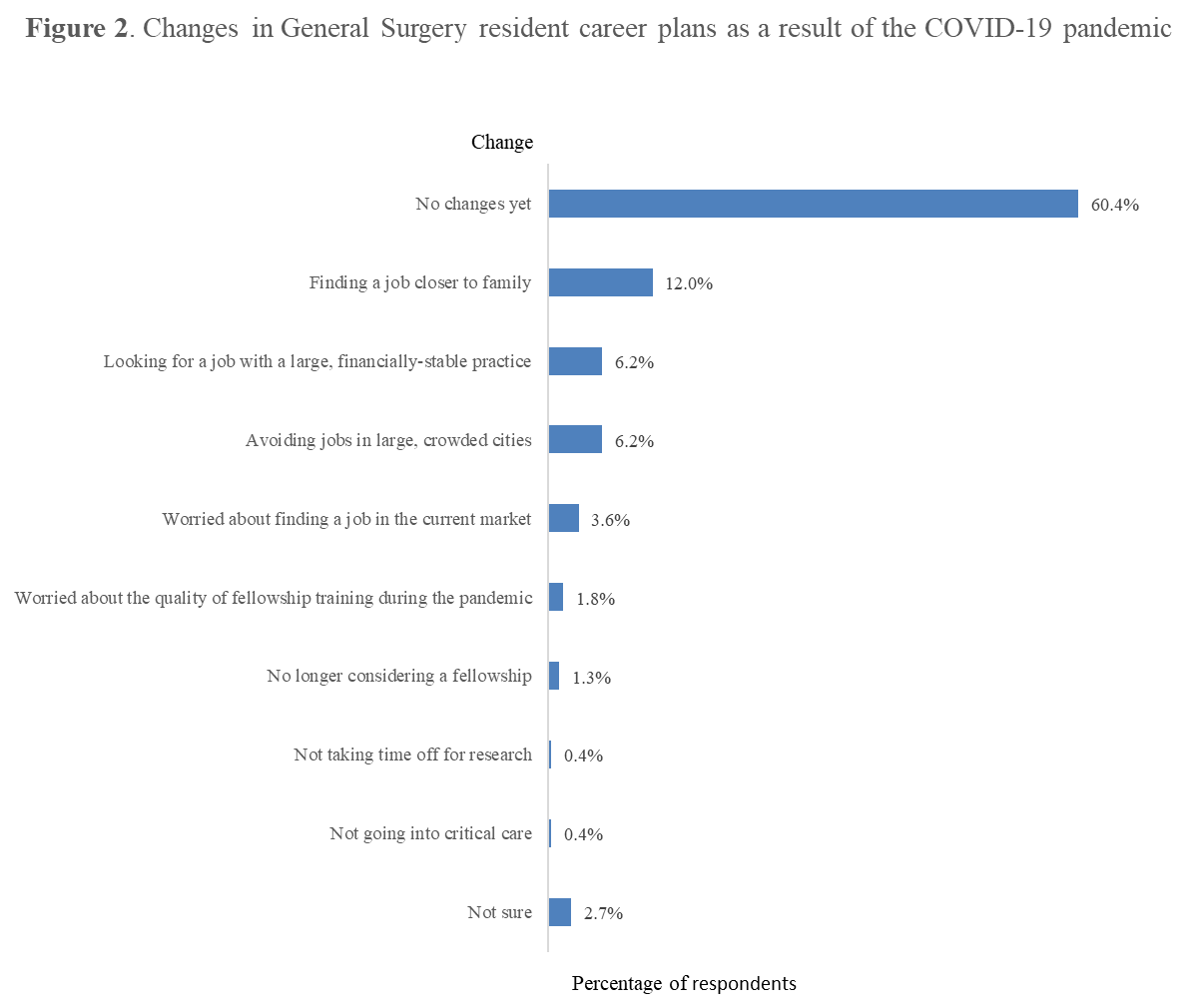
About one third of residents (34%, n=71) reported that the pandemic changed their career plans. Residents reported looking for a job closer to family (n=27, 13%), looking for a job in a large, financially stable practice (n=14, 7%), avoiding jobs in large, crowded cities (n=14, 7%), and no longer considering a fellowship (n=3, 1.4%), among other career changes (Figure 2).

Discussion
The results of this study suggest general surgery residents were financially impacted by the COVID-19 pandemic. A majority of respondents either indicated no changes to their financial situation or reported positive financial effects of the pandemic, such as decreased spending, increased saving, and receiving a stimulus check. However, approximately one-third of respondents indicated a negative financial impact resulting from the pandemic. Some of these effects, such as increased childcare costs, helping a family member financially and decreased or loss of partner income, pose potential financially devastating effects. Although many around the country have experienced these effects of the pandemic,11 they can be especially detrimental to our trainees given their low income and limited autonomy within the health care systems.
A number of respondents decried the absence of hazard pay as a mean to reduce the pandemic’s financial impact. The pandemic posed potentially harmful workplace conditions for healthcare workers, so the concept of hazard pay is an important issue. Hazard pay is defined as "additional compensation for performing duties that place workers in potentially dangerous situations.12 While there have been national calls for providing hazard pay to all essential workers during the pandemic,13 only 26% of employers surveyed in 2020 planned on providing hazard pay for their workers.14
Despite residents increasingly demanding hazard pay during the COVID-19 pandemic, hospitals have not yet addressed this issue,12 at a time when they are spending significant amount of money to recruit extra staff and provide hazard pay for physician assistants.15
The effects of the pandemic on the career plans of residents indicate a shift in their perspective. While approximately two-thirds of our respondents indicated no change in their career plans, those who did report changes indicated proximity to family, financial stability, avoiding lengthy additional training, and avoiding jobs in crowded areas as common reasons for their new career plans. These findings suggests that given the uncertainty brought by the COVID-19 pandemic, the general surgery residents are unsurprisingly prioritizing safety: the social safety of the family network, financial safety of large practices, and safety from coronavirus transmission in less crowded areas.
The current literature on general surgery residency and fellowship application trends is limited, but internal medicine has seen a more significant increase in fellowship applications. This was hypothesized to be related to the short-term job security in fellowship training, or the lower barrier to participating in a virtual application cycle.13
This study has several limitations. Given the voluntary distribution method by program directors, a response rate was not able to be calculated and the opinions of non-responders is unknown. Additionally, our sample was largely from residents training in the Northeast and Midwest, and as such, our results may not be generalizable to all surgical residents nationwide. However, the results were similar across geographic regions, suggesting that the results are likely reflective of the perspectives of surgical residents as a group. Furthermore, although we surveyed residents from multiple different institutions, we were not able to compare each program’s individual experience and response during the COVID-19 pandemic. Finally, the survey was administered during the first six months of the pandemic. As the COVID-19 pandemic enters its third year, the potential of it having a greater impact on financial wellness and career outlook is significant. Further studies are necessary to investigate how these impacts have unfolded throughout the pandemic.
Despite these limitations, this study illustrates how the COVID-19 pandemic has impacted the financial situation and the career plans of general surgery residents and identifies the need for better supporting our trainees during challenging times.
Conclusions
General Surgery residents have experienced significant financial difficulties and changes in their career plans during the COVID-19 pandemic. Therefore, comprehensive interventions from the Accreditation Council for Graduate Medical Education and residency programs are necessary to adequately support our trainees as essential workers during public health emergencies.
Disclosure
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.