
Background
Post-graduate resident physician curriculum is typically delivered as a combination of didactic lectures and experiential, direct patient care activities. However, this pedagogy has led to questioning resident engagement as well as knowledge acquisition and retention.1 This is particularly true regarding current generations of residents who prefer short blocks of learning material, or microlearning, and online digital resources for presentation of information.2,3
A flipped classroom may increase resident engagement since its pedagogy requires preclass assignments to successfully engage during in-class activity. Dedicated class time is reserved for problem-based, collaborative learning and advancement of concepts.4 The flipped classroom pedagogy theoretically improves content retention and a higher level of learning. Residents may better apply information, experience greater analytic skill to identify appropriate use of information, augmented ability to evaluate their knowledge application, and perhaps even demonstrate mastery by developing or researching methods for systems improvement.5,6
There are reports of flipped classroom benefits in several healthcare professional programs including medical school.7–9 Only a handful of reports in graduate medical education exist, and even fewer publications discussing application of flipped classroom in Otolaryngology-Head & Neck Surgery (ORL) post-graduate resident education.
Our aim is to share the experience through survey responses of a single ORL training program incorporating the flipped classroom method. We also discuss feasibility, resident and faculty perspectives, and lessons learned. We hypothesize that inclusion of flipped classroom pedagogy into didactic curriculum engages resident physician trainees and repurposes some faculty lectures.
Methods
Annual Program Evaluation. Residency programs annually conduct internal review by the Program Evaluation Committee (PEC) per the Accreditation Council for Graduate Medical Education (ACGME), the residency program accrediting agency that ensures professional education standards are met for physician trainees to deliver high-quality, safe medical care upon graduation. In 2018 our residents of the University of Mississippi Otolaryngology-Head &Neck Surgery program commented on the annual internal survey that they wished faculty lectures underwent improvement with addition of new material, removal of outdated items and complete overhaul of certain presentations. This critique precipitated PEC and department educational leadership to develop a program action plan of implementing flipped classroom method for some rhinologic and head and neck surgery topics in academic year (AY) 2018-2019.
The junior and senior level residents that participate in the PEC annual program review agreed that integration of formal flipped classroom format for some topics could improve various didactic presentations perceived as needing an update. Additionally, they felt flipped classrooms may engage resident learners through non-traditional, interesting encounters of new material for juniors, or review of the curriculum for seniors. Action plan areas for improvement is a requirement by the ACGME, and implementation of an action plan involves faculty and resident assessment. Therefore, our implementation of our flipped classroom action plan falls into the University of Mississippi IRB class of exemption.
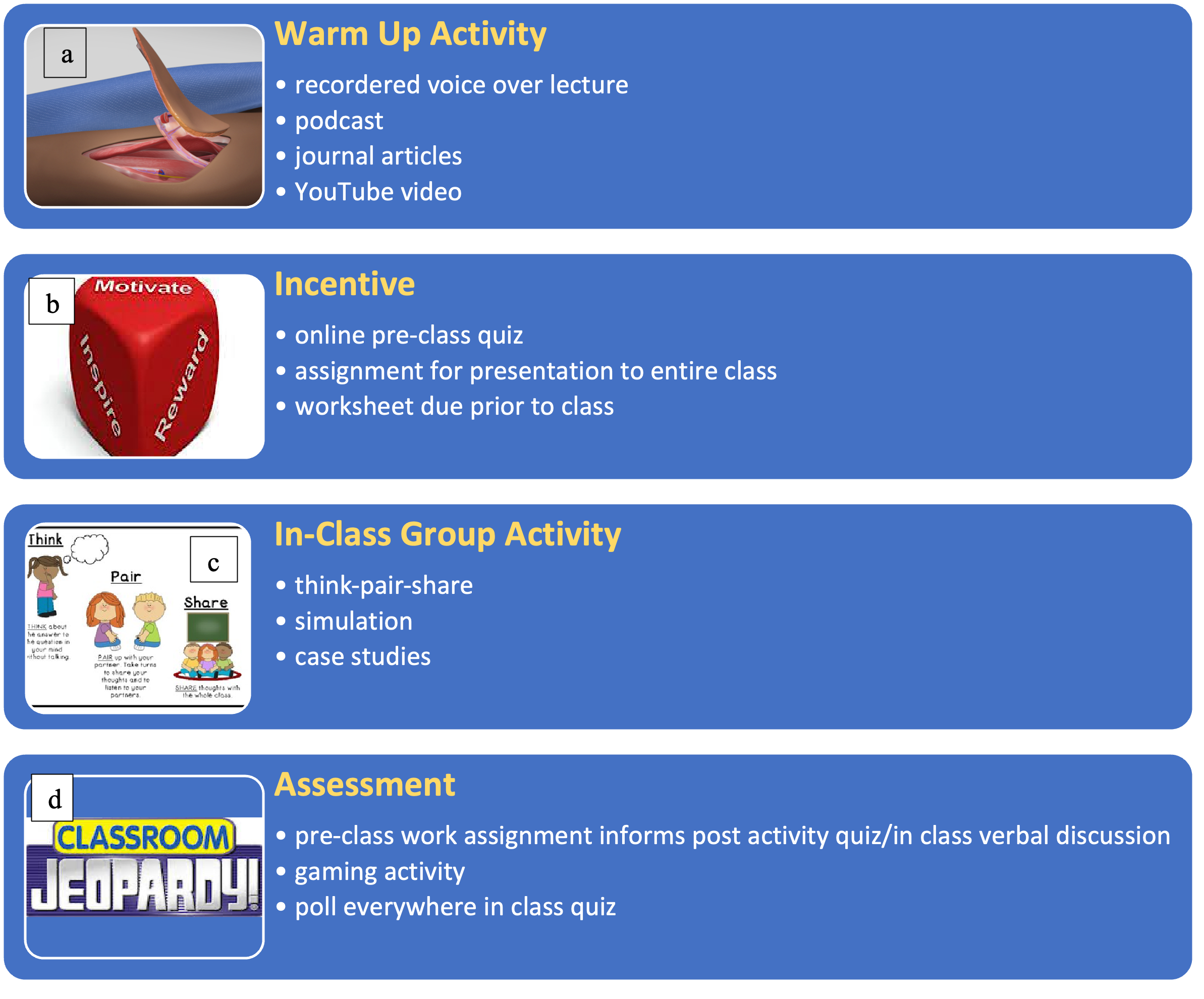
Faculty Introduction to Flipped Classroom. In AY 2019-2020, flipped classroom theory, rationale for use, key elements, and literature review were shared with all faculty. Our program goal for faculty was to collectively incorporate flipped classroom method into 30% of curriculum in AY 2019-2020 where at least 1 topic from each subspecialty was delivered this way. Flipped classroom involves exposing the learner to new subject matter prior to formal inclass instruction. The application and higher level of subject matter processing occurs during inclassroom activity. Key elements to delivering a flipped classroom include: a) warm-up activity,
b) an incentive to complete the pre-classroom warm-up, c) mechanism to assess knowledge at the conclusion of warm-up, and d) in-class activity to focus on higher level cognitive activities (see Figure 1).10 These key elements and specific tools to aid in creating a successful flipped classroom such as Nearpodâ and PowerPointâ voiceover, were shared with faculty. Our department Education Coordinator availed herself to any faculty member requesting assistance with technology for their specific flipped classroom.

Assessment. At the conclusion of AY 2020-2021 residents and faculty were surveyed [Appendix A1] regarding their experience with flipped classroom methodology and to assess benefits of incorporating this approach to curriculum delivery. The surveys administered were internally developed and specific to our residency program with no collection of validity evidence.
Results
Both resident learners and faculty members were surveyed via Microsoft Formsâ. Residents were queried on topics to assess their experience with flipped classroom, to consider preparation time, and appropriateness of topics covered utilizing flipped classroom to convey subject matter. Eleven of 15 residents responded. All post-graduate year 4 and 5 trainees responded while only 1 of 3 post-graduate year 3 trainees completed the survey. Overall, postgraduate trainees in years 1-4 had a positive experience with flipped classroom scoring better than neutral regarding “enjoy participation”, “overall positive experience”, “appropriateness for certain topics”, “increase knowledge application”, and “increase knowledge retention.” Twothirds of senior level residents in their 4th and 5th years of post-graduate training believed that the flipped classroom format required too much preparation time, as did 50% of interns that participated. No resident felt that subject matter covered by flipped classroom method was inappropriate. Some comments reflecting consideration of appropriateness of flipped classroom and overall utility are found in Table 1.
In AYs 2018-2020, there were 12 core Otolaryngology faculty. Faculty survey responses were provided by 5 of the 7 faculty who conducted flipped classroom. The residency program director and associate residency program director were excluded to minimize bias since they created the flipped classroom educational programming. Faculty disciplines who submitted survey responses included General Otolaryngology, Rhinology & Skull Base Surgery, Neurotology, and Plastic & Reconstructive Surgery. Excluded from survey participation, the residency program and associate program directors’ disciplines were both Head & Neck Surgical Oncology. Forty percent of faculty survey respondents believed development of flipped classroom for curriculum delivery demanded more time than typical PowerPointâ presentation.
Most faculty respondents (80%) either agreed, or strongly agreed with enjoying the flipped classroom experience. All faculty respondents understood the key components and rationale for producing a flipped classroom. One faculty member did not believe the flipped classroom experience was positive and 80% responded that the flipped classroom pedagogy should have a regular role in resident curriculum delivery. Faculty comments describing flipped classroom experience are found in Table 1.
Conclusions
Resident and faculty survey responses demonstrate that utilization of flipped classroom effectively delivered chosen didactic curricula and was feasible for our ORL training program. Overall, both resident physician trainees and faculty enjoyed flipped classroom delivery of subject matter chosen. Faculty understood the rationale and structure for creating a flipped classroom. Resident trainees understood their assignments, demonstrated responsibility in completing the assignment prior to the planned classroom activity, and understood the need for completion of pre-classroom work to fully participate and benefit in the assembled class learning event. Neither residents nor faculty felt too much extra time was involved in participating or preparing a flipped classroom event overall.
A concern raised by both a resident and faculty member was that the individual assignment for learners favors mastery of that specific assigned topic leaving the resident at a potential deficit with respect to the remainder of the lesson. Indeed, a threat to resident completion of pre-classroom warm up is time [see Figure 2]. Even with provision of the pre-class assignment 1-2 weeks in advance, residents must also balance on-call obligations, preparing for daily surgical cases, and remaining current with all other educational curricula. However, most Otolaryngology residents are likely compelled to not only prepare their assigned topic, but also to review other material outlined in the curriculum schedule for both traditional lectures and alternative classroom formats. In fact, the lead author’s experience with flipped classroom was that, on one occasion, a mid-level resident apologized to the residents during the in-class activity for not remembering to share his assignment. Following class, the resident immediately emailed the faculty member and residents his assignment to complete the comprehensive slide deck that resulted from the in-class activity for residents to review later if desired.

One opportunity of the flipped classroom model is the customizable nature of successful flipped classroom events [see Figure 2]. Customization allows the faculty members to create learning experiences specific to a topic. For instance, a topic focused on a surgical procedure may utilize an in-class simulation; whereas, a topic focused on clinical trial studies that impact head and neck cancer treatment may utilize in-class case-studies. Customization allows development of in-class activities that can optimize learner application and higher levels of learning. Opportunity lies in ability to test the theory that flipped classroom pedagogy increases knowledge acquisition and retention. Current methods of assessing resident physician trainee knowledge is largely based on standardized testing. The ability to test the theorized benefit of increased knowledge gain, retention, and application of knowledge is not suited for standardized testing. Rather, observation of resident application of knowledge is assessed in the operating room or in the management of patient consultations for example. The optimal next step is collaboration amongst residency programs to develop standardized flipped classroom scenarios for specific topics designed and implemented using the same key elements to better test the theory of higher learning benefit via flipped classroom pedagogy.
Another opportunity to enhance senior level resident experience is to lead in-class activities with the faculty member providing in-person support. Serving as the leader could increase senior resident demonstration of higher level of learning and engagement. On the other hand, senior level residents may feel they mastered the topics covered in the flipped classroom scenarios provided.
We recognize several resident educational benefits provided by flipped classroom [see Figure 2]. Active learning assignments, which are necessary pre-class to achieve a successful inclass experience, foster the requisite lifelong self-directed learning of physicians. Millennial generation trainees and after prefer accessibility of learning materials through online applications, available on-the-go. Residents can reference previously utilized course material for studying and reinforcement of knowledge, preparing for a difficult case, reviewing relevant material for specific surgical rotations. The flipped classroom model lends itself to the preferable learning pattern of today’s students, structured by interactive learning experiences delivered in shorter segments utilizing media such as videos and other technology-driven interactive formats.9 In-class engagement activities may also aid in developing a more reserved resident’s selfconfidence and ability to educate others – peers, students, consulting healthcare providers, patients and families.1,7
A primary threat to achieving successful flipped classroom learning experiences for Otolaryngology residents is their time. Time is also a potential threat to faculty preparing these educational events. The faculty member requires some creativity to envision an effective inclassroom event. The in-class event development dictates the pre-class learning materials and activities provided in advance. Effective flipped classrooms also require high-quality information technology. With assistance from our program’s education coordinator, we were able to navigate the use of Nearpodâ, create voice-over PowerPointâ that were prior presentations and deconstructed into smaller subtopics, and incorporate the American Academy of Otolaryngology’s appropriate FLEX (FLEX—Focused Lifelong Education Xperience) curriculum of surgical videos, webinars, online simulation and gaming modules, for example.
Our Otolaryngology trainee educational curriculum is delivered over a 2-year cycle. This construct permits faculty members to deliver a specific subject to each trainee twice during the residents’ tenure. We believe delivery of appropriately chosen topics can occur in the traditional format and in an alternative pedagogical form. Residents thereby encounter a variety of teaching methods that may further reinforce the subject matter, particularly since knowledge is acquired differently amongst individual learners and is further informed throughout training by experiential encounters.
One limitation of this study is that it represents the experience of a single residency program. This prevents generalizability to other training programs both within Otolaryngology and other disciplines. Customization of each flipped classroom event is attractive to make content delivery interesting and capture the audience. Customization minimizes comparison of scenarios to determine best practices. The authors believe that through collaboration with other training programs utilizing standardized flipped classroom content will allow evaluation of these limitations.
Summary
Flipped classroom is feasible, enjoyable and meaningful to participants of a single Otolaryngology-Head & Neck Surgery residency program. All subject matter necessary for resident trainees to become independent practitioners may not be amenable to a successful flipped classroom.
Author contributions
- Conception and design of study: GDJ, SPS
- Acquisition of data: GDJ, BJB
- Analysis and/or interpretation of data: GDJ, BJB, LLJ, SPS
- Drafting the manuscript: GDJ, SPS
- Revising the manuscript critically for important intellectual content: GDJ, BJB, LLJ, SPS
- Approval of the version of the manuscript to be submitted: GDJ, BJB, LLJ, SPS
Financial disclosures
The authors have no financial disclosures.