
INTRODUCTION
Teaching residents how to perform arthroscopy is an essential duty of all orthopedic residency programs. Previous literature has demonstrated that arthroscopic instruction of various styles can be very effective in developing arthroscopic surgical sk’ills; these include a typical mentor-based approach in the operating room, simulators that allow residents to gain experience in an artificial fashion before operating on a live patient, and cadaveric based labs.1–5
Augmented reality (AR) is a relatively new technology that has been increasingly implemented in the medical field.6,7 The principle of this technology is that it creates a unique visual experience by combining a digital workspace with the physical environment of the user, allowing images, information, or other digitally generated elements to be superimposed onto the user’s surroundings.3,5,7–13 The utilization of AR technology in surgical practice has included the use of smartphones, tablets, and even high dynamic range (HDR) AR glasses such as Microsoft HoloLens and Google Glass.5,7–13 Total knee arthroplasties have seen the beginnings of AR navigation in orthopedic surgery through high-precision holographic guidance utilizing AR glasses.9 AR glasses and displays can be used to provide lesser-experienced surgeons with guidance from specialists at a remote location through voice and visuals.7,8,12
The purpose of this study was to evaluate the experience of orthopedic residents during arthroscopic instruction using augmented reality with in person and remote instructors.
METHODS
This study was approved by our institution’s IRB. At one of the institutions involved, we conduct resident arthroscopic instruction with regular cadaveric labs; a total of 8 labs per year with 4 labs focused on knee and 4 focused on shoulder arthroscopy. Residents receive instruction at a lab station with one other resident. The labs are conducted over 3 hours in a skills lab.
During the 3-hour program, the residents underwent learning that included instruction using AR technology. All included residents (post graduate year 3-5) have previously undergone the same lab based arthroscopic instruction without the use of AR instruction. The AR technology allows for interaction or instruction from someone removed from the surgical table, such that the remote instructor can introduce their hand or other instruments into the projected arthroscopic monitor image. The arthroscopic image was projected onto two monitors, one with a standard image, and one with an AR image (Figure 1). The AR image was generated via internet connection through two iPads using a free app called HelpLightning. In the laboratory, one iPad, which is running the AR platform, is videotaping the non-AR monitor. It is then connected to the to the second monitor, such that the second monitor displays the AR image. On the remote side, a second iPad is placed facing a white background; anything can then be placed into the field of view from the iPad camera, between the camera and the white background, such that it gets projected into the AR image generated via the platform. This is then viewed on the AR monitor at the local site.

A total of 15 residents were instructed by a remote surgeon at an institution roughly 1,000 miles away; an educational experience that was completely dependent on the AR application. An additional 15 residents were instructed through AR by an onsite instructor who was removed from the laboratory table but would allow verbal interaction that did not rely on the AR application. The residents were remotely instructed how to perform arthroscopic procedures including diagnostic arthroscopy, partial meniscectomy, anterior cruciate ligament reconstruction, biceps tenotomy, subacromial decompression with acromioplasty, distal clavicle resection, and rotator cuff repair.
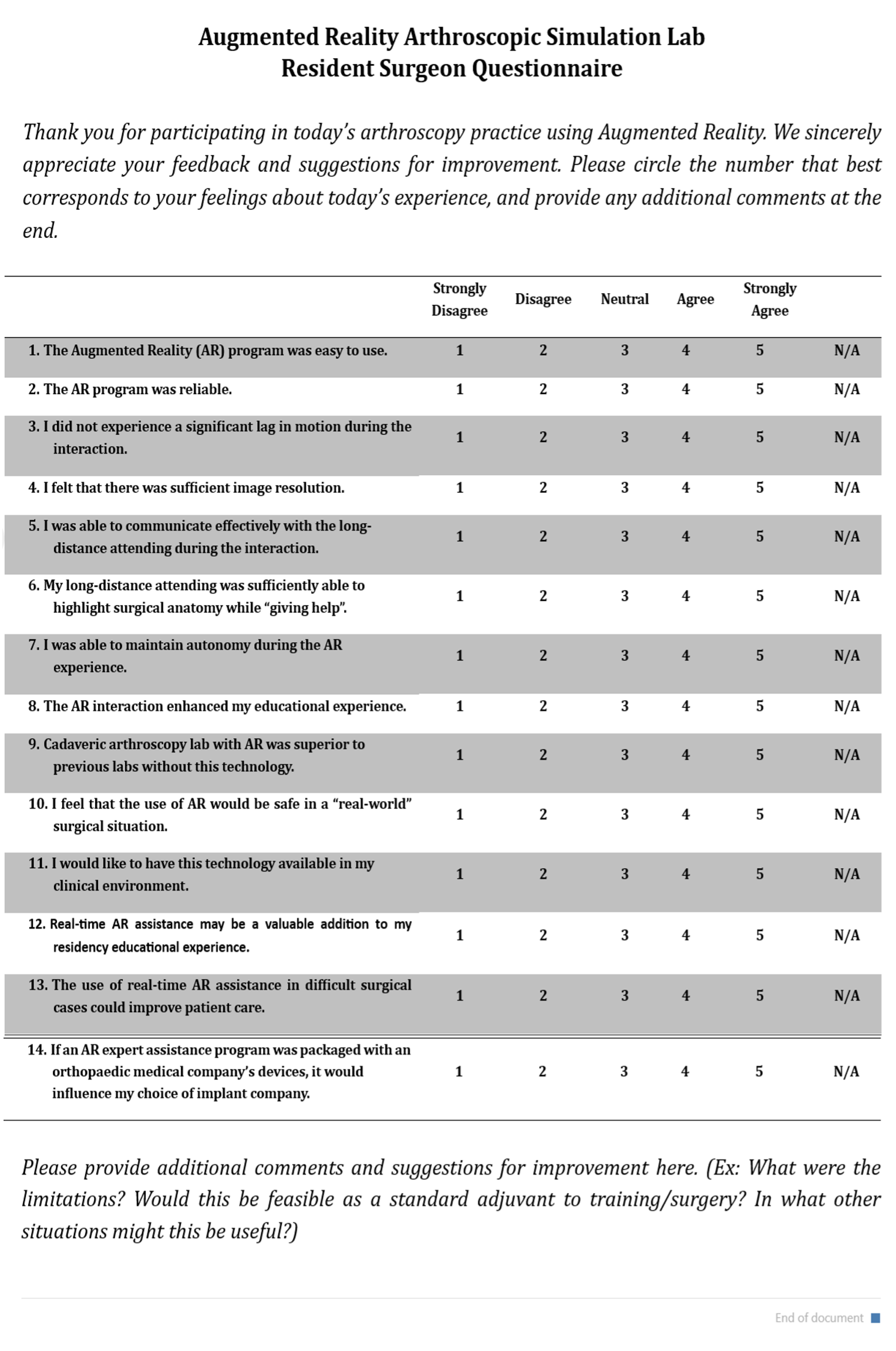
Immediately following the laboratory program, the residents completed a 14-question Likert scale survey about their experience with AR (Figure 2). For each Likert scale question, scores were 1-Strongly Disagree, 2-Disagree, 3-Neutral, 4-Agree, 5-Strongly Agree.

Statistical Analysis
All surveys were scored, and the mean and standard deviation were calculated. Paired student’s t-test was used to compare the results between remote and onsite AR instruction.
RESULTS
The overall results are displayed in Table 1. There were no significant breaks in the instruction provided during the procedures. The residents were able to complete all procedures conducted through AR teaching.
The comparison between remote and onsite instruction is displayed in Table 2. The only questions that presented significant differences between onsite and remote labs were questions 3 and 10, regarding lag in motion of the interaction and the resident’s perceived safety of AR use in a “real-world” surgical situation, respectively.
DISCUSSION
This study provides information about the possibilities of using augmented reality for remote arthroscopic instruction. The use of AR technology was well received by the residents, highlighted especially by maintenance of autonomy, and can serve as an additional tool for arthroscopic instruction. With only a couple exceptions, there was not a difference between remote and onsite AR instruction. There is room for improvement in the technology itself, both hardware and software, that could improve connection and image resolution.
The responses and experiences by the residents involved in this study suggest that the use of AR technology can be effectively utilized to provide arthroscopic instruction. This can build upon the laboratory based arthroscopic instruction already provided to residents in many areas. This could also be expanded to help improve arthroscopic knowledge and skills for providers already in practice. There are some material resources needed to implement the technology including portable devices and connecting cables, as well as tools to hold the devices; use of the AR application also requires some technical knowledge. Despite this, the technical knowledge and material resources required are relatively minimal, and therefore should allow the concept of AR arthroscopic instruction to be easily implemented.
It is important to know whether the technology can be used for both local and remote teaching. The comparison between onsite and remote AR instruction demonstrated minimal difference, with the only differences being the only differences being in the observation of a lag in motion and with the perceived safety of AR in a “real-world” surgical situation. Thus, the results suggest that the technology can effectively be used for both in person and remote instruction.
The survey results do suggest that there is room for improvement in the technology, both in audio and visual quality, and overall performance. Despite the fact that no procedures were negatively impacted by the use of AR instruction, there were times were there was a slight lag in the connection for the AR instruction, delaying the instruction slightly. There was also occasional difficulty with the residents being able to hear the remote audio; this was ameliorated by connecting speakers to the iPad in the laboratory. A higher image resolution could be obtained by altering the methodology and directly porting or streaming the collected non-AR video to the non-AR monitor and the instructor’s iPad simultaneously. This would eliminate the need for the first iPad, which likely altered the original video’s image resolution due to a difference in scan rate and/or pixel count.
Limitations in this study include the possibility that it is underpowered to detect a difference between remote and onsite AR instruction. Another limitation is that there is no non-AR control population; and the survey is such that it is impossible to ask the same survey questions to residents not undergoing AR instruction. All included residents, however, have previously undergone the same lab based arthroscopic instruction without the use of AR instruction, and the survey asks them to compare the AR instruction to previous non-AR experiences.
It is likely that AR technology can be applied in other surgical settings, and perhaps even more broadly into multiple medical applications in order to improve medical education, which in turn can translate directly into improved patient access and care.
CONCLUSION
The use of AR technology was well received by the residents and can serve as an additional tool for arthroscopic instruction. There is room for improvement in the technology itself in terms of better connection, as well as audio and visual quality. It may be possible to increase the reach of arthroscopic instruction through the use of remote teaching tools. Augmented reality applications offer an exciting opportunity for remote arthroscopic instruction and possibly for broader medical education.
ACKNOWLEDGEMENTS
The authors wish to acknowledge Megan Reams, Kelsey Schnackenberg, Scott Houlihan, Slava Yarmakovich, and Bruce Leonard for their assistance in making it possible to have the equipment (iPad and cables) and establish the appropriate connection via the AR platform.
Funding Disclosure
The author(s) declare that they have no conflicts of interest.