Introduction
As the COVID-19 pandemic peters out,1 travel and social restrictions have been all but lifted. This includes the work environment with organizations dialing back on the remote work arrangements that was enforced during the pandemic.2
In the healthcare sector, numerous para-clinical activities which had shifted to the online space, are returning to the in-person format to varying degrees. These include tumor boards, journal clubs, multi-disciplinary meetings, educational webinars, and the morbidity and mortality conferences (M&M).
The M&M is a hallowed regular gathering of practitioners in many surgical units, serving as an audit and educational tool.3,4 The abrupt transition of the M&M to the online space at the start of the pandemic, and its gradual return to the in-person format, gave surgeons a unique opportunity to experience and compare both methods of conduct.
Anecdotally, opinions about the effectiveness of the online format ranges widely. Some deem that the online format erodes the cohesion, accountability, and discipline that the in-person format seeks to instill. Others opine that the online format improves attendance and promotes better communication and learning.
The aim of this study is to investigate the opportunities and challenges, as well as the learning advantages, associated with the online and in-person M&M within a single surgical department. Based on the knowledge obtained from the study, recommendations are made for a way forward, where desirable aspects of both formats are combined into the future conduct of the M&M.
Methods
This study was carried out within a single surgical department, based on a self-reported questionnaire. All staff in the department, 130 in the department emailing list (clinical staff n=113, administrative staff n=17), were included in the survey. This study was exempted from review by the Institutional Review Board (IRB).
The conduct of the M&M conference within this center takes place every Friday morning. All mortalities and unplanned returns to the operating theater in the preceding week are presented. Other presented cases include significant morbidities or those of surgical interest. These would have been flagged up by the Head of Department in advance so that the surgeons have time to prepare their presentations. Discussions are moderated by the Head of Department. The above agenda is the same for both the online and in-person formats.
The online survey was crafted using FormSG, a free digital form builder tool that enables public officers in Singapore to create and store digital forms in a secure environment. The research project was advertised during a M&M conference and staff were encouraged to respond on a voluntary basis. This was followed with an invitation to participate, with the link to the survey questionnaire circulated twice within a period of 4 weeks (30 Mar 2023 – 30 Apr 2023) via email and WhatsApp messages. At the end of this period, the data from the online questionnaire were extracted for analysis using MS Excel. The manuscript was prepared using the SRQR (Standards for Reporting Qualitative Research) framework for qualitative research.5
Survey Questionnaire Design
The web-based questionnaire comprises 17 questions and captures responses using a mix of best single answers, dichotomous and rating scales (Likert), and open-ended answers. Per IRB requirement, a participant information sheet informs all respondents the purpose of the study, the voluntary nature of the participation, and that implied consent was assumed when the participants submit their responses. The questions were crafted by the authors to assess whether the participants favored one modality over the other, the reasons for their preferences, and explored some practices which were hitherto less described e.g. the proportion of participants who engaged in non-M&M related activities during the online M&M, whether these activities distracted them from the main discussion. The survey was developed by the principal investigator and evaluated by three test subjects (co-PI and two other senior consultants within the department) prior to the actual administration. The survey took approximately 5 minutes to complete and was completely anonymous. The survey questions are appended in Appendix A as supplementary data.
Results
A total of 67 staff completed the survey, giving a response rate of 51.5%. The demographics of the respondents are outlined in Table 1.
All participants (n=67) responded that they have experienced both the in-person and online formats. With online M&M (OM), most responders (n=42, 62.7%) indicated they were more likely to be punctual for OM.
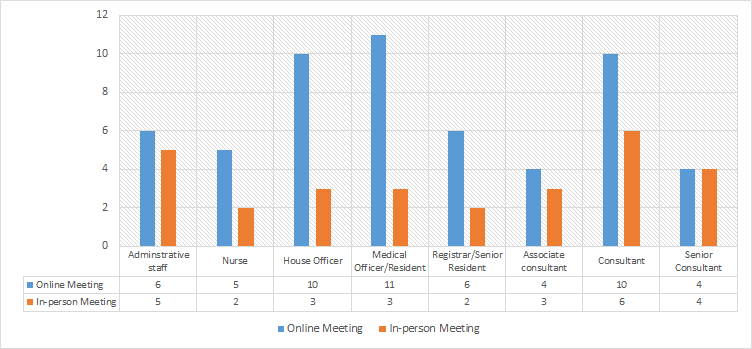
It was observed (from Figure 1) that OM can increase multi-tasking activities, with 56 (83.6%) of staff engaged in non-M&M related activities such as emails, ward rounds, reading other papers, commuting, etc. This is opposed to the physical in-person M&M (PM), where only 28 (41.8%) were engaged in other activities like replying to emails, reading the news on their mobile phone, etc.

It was interesting to note that of those who admitted to engaging in non-M&M activities during OM (n=56), most did not consider these activities as distractions (n=41, 73.2%). Instead, they opined that they were able to multi-task and considered this an optimal use of their time while participating in the OM. The rest (n=15, 26.8%) acknowledged that these non-M&M activities were distracting but still engaged in them because OM allowed them to do so discreetly. Specific responses from this group include “heavy clinical workload”, n=5; “selective interest in M&M cases”, n=1; “commuting and being able to sleep in”, n=1; “short attention span”, n=1.
Unfortunately, only a minority responded that they were fully focused during OM, i.e. they do not engage in non-M&M activities during OM (n=11, 16.4%). The reasons were related to a desire to learn, mindfulness, and being present and focused.
The reasons for favoring or liking OM are ranked in the following order (participants can choose more than one option). The top reason is the convenience which facilitates remote attendance and multi-tasking (n=46, 68.7%), other reasons include the use of the chat function which allows for side or private conversations without interrupting the main presentation (n=27, 40.3%), being able to hear better (n=26, 38.9%), more cordial/ less heated discussions (n=25, 37.3%), and less stressful when presenting cases online (n=23, 34.3%).
On the other hand, the reasons for favoring or liking PM can be ranked in the following order. The highest (n=30, 44.8%) is the social need of seeing colleagues in person, followed by engendering better departmental cohesion and a greater sense of accountability (n=21, 31.3%), a greater focus at physical meetings 19 (28.4%), and residents being able to practice public speaking (n=17, 25.4%).
When asked to decide the way forward, a minority (n=11, 16.4%) wanted a complete resumption of the full physical in-person M&M, a significant number (n=20, 29.9%) wished for the fully online M&M, while the majority (n=36, 53.7%) wanted a hybrid format. See summary in Table 2.
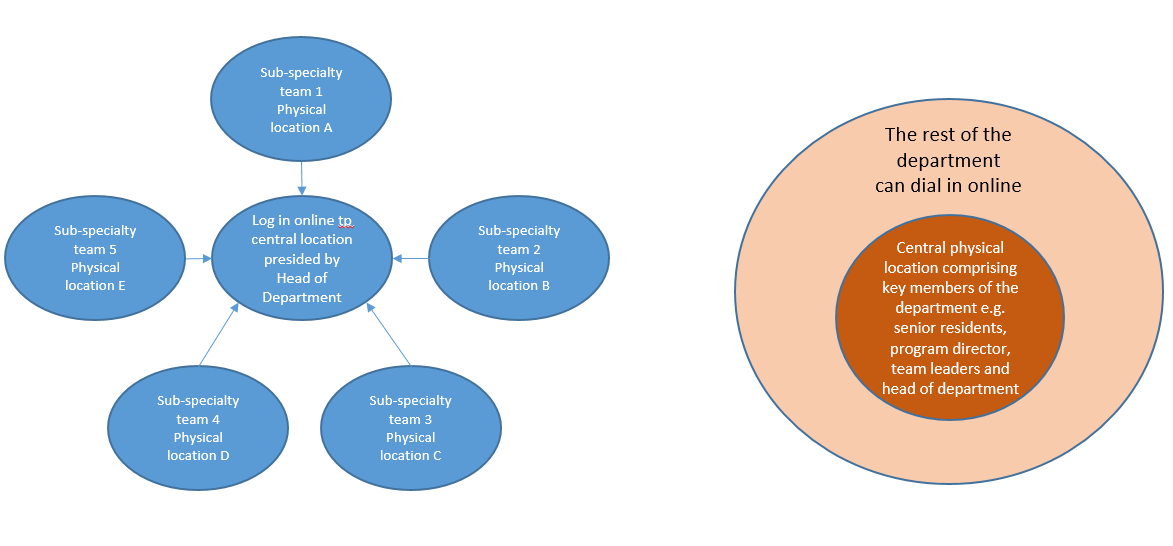
For those who wanted a hybrid format, the majority (n=26, 72.2%) wanted a system where a physical in-person M&M is conducted once a month, with the rest of the weekly M&M conducted online. Other hybrid forms proposed include a laissez-faire style, where whoever wants to turn up physically may do so, while the rest continue to turn up online; a subgroup of people (the chiefs of each subspecialty team and the general surgical residents) turns up physically, while the rest turn up online; everyone turn up physically but at different locations with their subspecialty teams, and these teams log onto the main M&M online discussion.
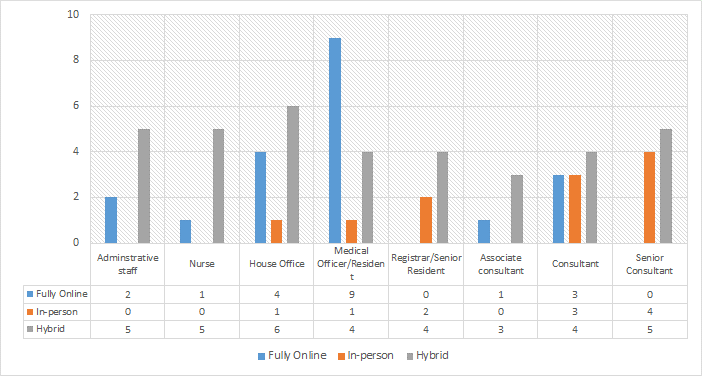
Those who voted for fully online M&M, 13 out of 20 (65%) are the junior staff (HOs and MOs/ residents) as shown in Figure 2. On the other hand, 7 out of 11 (63.6%) who voted for the fully in-person format are senior consultants and consultants.

Discussion
The M&M is an important tool in surgical departments where surgeons learn from each other.6 In this center, the M&M has always been organized in the physical in-person format, steeped in traditions with specific seating arrangements and order of presentation. It was something that generations of surgeons were familiar with. At the beginning of the COVID-19 pandemic, the M&M was shifted online in tandem with numerous other paraclinical activities. It is not clear if the shift has resulted in any change to the quality of learning. It is even harder to attribute any differences in patient outcome to this change in M&M format. Instead of outcome indicators, this survey sets out to measure and describe the process indicators, which may inform leaders of surgical departments as they continue to evolve the conduct of the M&M in the post-COVD era.
The findings from this survey are not surprising. Intuitively, leaders already knew that online meetings cannot match in-person meetings in terms of the attention they engender from participants. Hitherto undescribed, this anonymous survey was able to elicit candid responses that quantitatively measures the difference (83.6% OM versus 41.8% PM engaged in non-related activities). It may be alarming if we assume that engaging in non-related activities is the sole proxy measure of the quality of learning. Using this line of argument, if surgeons are not paying full attention, they do not learn from the highlighted mistakes. If this were the case, OM has no place in the surgical education toolbox. However, it would be premature to dismiss OM completely, throwing the baby out with the bathwater. The survey highlighted several OM benefits and learning advantages. Convenience reasons aside, surgeons reported improved punctuality, and benefits which are related to better communication, which by inference, lead to a higher quality of learning. These include better access to the conversation, e.g. “I can hear the discussions better”. In OM, everyone is accorded a front row seat figuratively, whereas in a typical in-person format, the back row participants may be less engaged with the conversation on stage. Moreover, the subsequent case discussion around the room following the main presentation is less audible if the microphone use is not mandated.
The survey also found that OM tends to be “more cordial, and less likely to be heated”. It is well known that rigorous discussions during PM can invoke strong emotions which may be counterproductive to learning.7 During OM, comments are usually made sequentially, rather than concurrently, i.e. people are less prone to talk over each other during OM, perhaps because it is technically harder to do so. One responder noted that OM discourages “people talking at the same time”. This OM feature of sequential comments has inadvertently promoted more “listening”, to balance the “speaking” component of a good conversation.8
Another benefit that respondents noted with OM is the chat function. This allows participants to share their views (along with links to articles and journals) with the main M&M, without interrupting the main oral presentation. The chat function also allows participants to chat with selected colleagues privately. These features promote good conversations at various levels, in accordance with the learning needs of the participants. E.g. a resident who is embarrassed to ask a question openly during PM, may be more inclined to ask a trusted mentor using the chat function during OM.
Additionally, participants like OM because it is less stressful to present cases online.9 OM does confer some degree of anonymity, which helps with stage fright. However, while this is beneficial in the short term, it does deny residents the stage to practice their public speaking, which will put them in good stead for the longer term.
There are also numerous PM positive attributes and learning advantages that respondents highlighted. A significant proportion responded that they like PM simply because they “get to see colleagues in person”. This reflects the basic need for social interaction especially in a department that typically thrives on teamwork.10 Some also reported that they are more focused during PM, which is supported by the finding in figure 1 where more people engaged in non-M&M activities during OM.
Others believe that PM being more onerous, it engenders a greater sense of cohesion and accountability. This may be inferred from the finding that most respondents reported a higher rate of punctuality with OM, and by inference, it takes less effort to be punctual for OM than PM. Moreover, with the anonymity conferred by OM, participants are held accountable to a lesser degree, allowing them to engage in non-M&M activities during OM, which include doing ward rounds, emails, and commuting.11
The attributes for both modalities should not be analyzed with the intent to extol one over the other, but rather, for both to be considered complementary so that surgical departments can decide on the way ahead for the conduct of the M&M conference. The majority responded that they would prefer a hybrid model for future M&M and defined the hybrid model as one that alternates between a fully PM (once a month) with the rest being fully OM (the remaining sessions for the month). It is noted that there are other possible hybrid models which may harness the positive attributes for both modalities. See Figure 3.

Of the group that voted for a full online M&M moving ahead, it is reasonable to conclude that this group, comprising mainly junior staff, is one that is saddled with much of the daily clinical tasks, and would appreciate the online format which gives them the opportunity to multi-task. They are also a digital native group familiar with the online format.
Of those who favored a full physical in-person format, these are mainly senior clinicians who, apart from being more familiar with this format, may be more vested in department’s overall direction and culture. In addition to the technical learning advantages for PM, it is likely that this group values the greater sense of accountability and cohesion that PM fosters. It may even be said that this group is likely to value more the teaching and modeling of the profession of surgery through the physical in-person M&M, the commitment in time and energy to the importance of this learning tool, and the ability to read body language, assess presentations, and offer real time discussion and disagreement.
This study is limited by the response rate. Without a tangible incentive for survey completion, the 51.1% response rate is acceptable, but not ideal.12 This being a single department survey is also limited by its generalizability to other departments. The authors were not able to perform stratified analysis because the numbers in sub-populations are too small for meaningful analysis. Finally, the survey was designed during the peak of the pandemic when the department was conducting the M&M fully online. However, when the survey was eventually administered, the department had already shifted to a hybrid model of one PM per month. This could result in a status quo bias when the survey asked for the preferred mode of the hybrid model.
Conclusions
The M&M is but one of many paraclinical activities shifted to the online space during the COVID-19 pandemic. As the pandemic ended, the manner with which these activities return to their physical forms is marked by heterogeneity, which could be the result of a paucity of published literature on this phenomenon. It is hoped that the attitudes and beliefs from this single center survey study will help surgical departments, and the leaders of other paraclinical activities, better understand the strengths and limitations of each modality, and aid them in the design of future meetings. Ultimately, a well-designed M&M is a key enabler for peer learning amongst surgeons, which by extension, leads to better patient care.